Photo credit: Kelly James
On International Day of Persons with Disabilities, we recognize the opportunity that the pandemic affords us to consider how we build back better. In this case, better means delivering more inclusive and accessible water, sanitation, and hygiene (WASH) services for people of all ages and abilities. At CAWST, we are committed to learning about how to design more inclusive WASH programs. During our semi-annual Learning Exchange and over lunch and learns, we have the great opportunity to invite experts from across the sector to help us consider how we can address gender, age, and disability more meaningfully in our work. One of the experts we heard from was David Achuroa. Today, we are pleased to welcome David to our blog. David is a WASH consultant and researcher, who specializes in inclusive WASH. Thank you, David, for sharing inclusive WASH knowledge with us!
The UN defines disability to include “long-term physical, mental, intellectual, or sensory impairments which in interaction with various barriers may hinder [a person’s] full and effective participation in society on an equal basis with others” (UN, 2007, pg 4). The World Health Organization (WHO) reports that there are 1 billion people with disabilities: 800 million of them residing in low- and middle-income countries (WHO, 2011). Statistic Canada estimates that 13.5% of Canadians aged 15 years or older have a disability (Statistics Canada, 2013).
My interest in disability issues runs deep. Throughout my academic and professional career, I focused my research and work on disability and disability practice in Ghana. I hold a Master of Arts in Social Anthropology from the University of Calgary, and a Bachelor of Science in Community Nutrition from the University for Development Studies in Tamale, Ghana. In research and community development programming, I try to apply what I learned to develop capacity of leaders to recognize and include persons with disabilities and their families.
But my passion for disability issues long predates any academic or professional engagement with the topic. Before all of this: I am, myself, a person with a disability.
In Northern Ghana in the 1980s, I was born in a rural village into the household of a smallholder farmer in the middle of a poliomyelitis epidemic. Unfortunately, as I was just learning to walk, I contracted the virus and became paralyzed in my legs. Until I was 10 years old, I didn’t have access to crutches or any assistive devices, so I would get around by crawling, or being carried by family members.
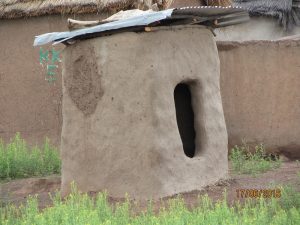
 -Entrance of a school toilet. Credit: David Achuroa
-Entrance of a school toilet. Credit: David AchuroaThroughout my childhood, sanitation facilities were poorly adapted to my needs, and were often virtually inaccessible. I would have to crawl on my hands and knees inside dirty latrines, when I wanted to use the toilet. Handwashing stations were out of my reach and unusable. The conditions were often so bad that I would prefer to practice open defecation; opting to use nearby bushes, risking attack by dangerous bugs and reptiles.
The toilets available at school weren’t any better adapted. Once I received assistive devices, I still wasn’t able to safely enter the latrine because they lacked a ramp, and adequate space and supports to move around safely once inside.
As you can imagine, this had a profound effect on my health, my confidence, and my relationship with others.
I was excluded from many social events and traditions. Children in the village eat together, out of the same bowl, using their hands, participating in a practice that is thought to encourage sharing and instill a sense of togetherness. I was often considered dirty and undeserving of sharing in the same bowl. It was incredibly isolating and I felt totally alone. I thought these problems were unique to me.
When I started working with people with disabilities and their families, I realized I was not alone. When I travelled outside of my village for school, workshops, and trainings, I saw that it is not only washrooms in my community that are inaccessible, but most sanitation facilities I encountered were similar; inaccessible, dirty, and impossible for me, and others with mobility impairments, to safely use.
The need to use the toilet still evokes feelings of insecurity and anxiety well into my adult life because of the uncertainty of whether or not I will be able to access the toilet and the consequences this can have on my dignity. I find myself wishing that I could travel without ever needing to use the washroom.
 -Entrance of a household toilet. Credit: David Achuroa
-Entrance of a household toilet. Credit: David AchuroaWhile working for a community-based rehabilitation program in Ghana, the people with disabilities whom I encountered expressed similar experiences and challenges. I heard stories of the economic impacts of inaccessible water, sanitation, and hygiene facilities, and the resulting negative health outcomes they regularly faced. I heard about the time costs they struggled to manage: mothers of children with disabilities reported having to manage their children’s complex sanitation and hygiene needs without adequate facilities or sufficient water. This is another time-consuming chore to add to the impossible list of domestic responsibilities. I also heard stories about the stigma, shame, and embarrassment of not being able to enter a toilet without help or without getting dirty.
Persons with disabilities are disproportionately affected by poor water, sanitation, and hygiene. Data from 34 European countries and Turkey suggest that persons with disabilities are twice as likely to lack a bath or shower in their homes as people without disabilities (UN, 2018). A disability report in Edmonton gives an overall 23% disability accessibility score after assessing public spaces such as parking, bathrooms, telephone, locker rooms, and showers (The Steadward Centre for Personal & Physical Achievement, 2015).
Disability accessibility is even more precarious in low- and middle-income countries. In Brazil, 97% of the primary schools have a toilet within the building, but less than half of these facilities were accessible to pupils with disabilities (UN, 2018). Likewise, in Bulsa District in Northern Ghana, only 19% of public toilets were accessible to persons with disabilities (PCBR, 2017).
Understanding how to improve access to inclusive water, sanitation, and hygiene requires an understanding of the barriers that prevent access. Barriers to the full and meaningful participation of people with disabilities in all aspects of life, including water, sanitation, and hygiene can be broken down into four broad categories: attitudinal, institutional, environmental, and communication.
Attitudinal barriers encompass harmful social norms, cultural beliefs, prejudices, and behaviours. They often stem from a perception that disability is a medical problem, requiring charity and pity. I see this barrier expressed in a range of ways, from patronizing ideas of what people with disabilities can and cannot do, to beliefs that disability is a curse, a dangerous spirit inhabiting a person’s body, as was the case in communities near to where I grew up. It also includes behaviours such as preference to use the disability designated toilet room instead of the regular toilet rooms because it is spacious and convenient.
Environmental barriers include features of natural or built settings, or the way things are constructed. Traditional designs of washrooms have largely neglected users with reduced mobility and other bodily differences. Latrines, tap stands, and handwashing facilities need to be properly and safely sited and easy to approach, free from obstacles or hazards, have facilities in place to support access (like ramps), and be equipped with the necessary space and supports to ensure users with diverse needs are able to use them. However, this is still often not the case. As a result, in more than 25 years of using a pair of crutches and braces, the struggle to access washrooms hasn’t improved much.
Institutional barriers include laws, policies, programs, as well as lack of data and standards. It is the conscious awareness of institutions to consider how their policies and programs impact populations with disabilities. Unfortunately, people with disabilities are often underrepresented in research and data, in decision making positions, and in consultation on policies or programs. The barriers also relate to the pace at which organizations formulate and adopt disability legislations, policies, and programs and take actions to remove attitudinal and environment barriers.
 -Imagine sitting in a wheelchair and trying to reach for the soap dispenser and tissue paper. Credit: David Achuroa
-Imagine sitting in a wheelchair and trying to reach for the soap dispenser and tissue paper. Credit: David AchuroaCommunication barriers refer to the lack of accessible, clear, and simple messages. This also includes the lack of inclusion of imagery of people with disabilities in hygiene promotion campaigns. Behaviour change campaigns, and promotional materials, rarely feature diverse images or representation of persons with disabilities or other diversities. In addition, braille writing on hygiene education is limited and hard to find, as are sign language interpreters in hygiene campaigns. Moreover, there are directional signs and symbols to show where to locate washrooms in buildings, but these signs are inaccessible to people with poor sight.
It is important to emphasize that these challenges and barriers cannot be dismissed as exclusive to “developing countries”. These barriers are common in our own communities, right here in Canada. Recently, I was dining out in a restaurant Calgary and when I wanted to use the washroom, I had to struggle down a steep and narrow staircase to access it. It was clear to me that a customer using a wheelchair would be completely unable to independently use this washroom. This situation is not uncommon; on more than one occasion, I have watched wheelchair users unable to reach sinks or handwashing facilities.
So, what can be done? Here are five tips on how you can start thinking about inclusion and accessibility in your WASH programming:
- When designing WASH programs, think broadly about of all the diverse users your initiative will include or impact. Seek to understand their unique challenges, needs, desires, preferences, and experiences.
- Gather and share data about disability in your WASH programs. Increased access to data will help raise awareness and can be used as a basis for designing more effective policies and programs in the future.
- Include people with disabilities in all phases of your WASH project; from consultation, planning, and budgeting, to implementation and evaluation. As the saying goes, the person wearing the shoe knows where it hurts the most.
- Look for opportunities to apply innovations to promoting accessibility and inclusion. New digital technologies such as Siri, Alexa, and voice speakers (used in elevators) can be explored for their usefulness in adding audio features to signal stations of hand sanitizers, soap dispensers, paper towels, and hand dryers for people with a visual disability. Innovations should be tested by users with different impairments. The inclusion of persons with disabilities at different stages of product development allows for proper adjustments and accommodation, before mass production of the technology and service.
- Policy makers, WASH practitioners and other WASH stakeholders should make a point of seeking out and participating in training courses on disability inclusive practices. We are also responsible for championing inclusion and accessibility.
To connect with David and learn more about his work, please reach out.
References
PCBR. (2017). Status of disability accessibility in Bulsa North District. unpublished
Statistics Canada. (2013). Disability in Canada: Initial Findings from the Canadian Survey on Disability (Catalogue 89-654-X, no.002). Ottawa: Ministry of Industry.
The Steadward Centre for Personal & Physical Achievement. (2015). Fitness Centre Accessibility Audit Summary Report. Edmonton.
United Nations. (2007). The convention on the rights of persons with disabilities.
United Nations. (2018). UN Flagship report on disability and development 2018. United Nations Department of Economic and Social Affairs.
World Health Organization. (2011). World report on disability. Malta.




 -Dalia’s impact goes beyond her community of Confuso. She has presented her experienced and advocated for rural communities at events with the Ministry of Agriculture and the United Nations Food and Agriculture program.
-Dalia’s impact goes beyond her community of Confuso. She has presented her experienced and advocated for rural communities at events with the Ministry of Agriculture and the United Nations Food and Agriculture program.

 -Sabuna Gamal works towards SDG 6: Safe water and sanitation, as well as SDG 5: Gender equality in Nepal. Photo credit: ACGC.
-Sabuna Gamal works towards SDG 6: Safe water and sanitation, as well as SDG 5: Gender equality in Nepal. Photo credit: ACGC. -Yashi works towards SDG 6: Safe water and sanitation and SDG 5: Gender equality in India. Photo credit: ACGC.
-Yashi works towards SDG 6: Safe water and sanitation and SDG 5: Gender equality in India. Photo credit: ACGC. -Thomas works towards SDG 1: No poverty, along with SDG 6: Safe water and sanitation and SDG 5: Gender equality on the CAWST team in Canada. Photo credit: ACGC.
-Thomas works towards SDG 1: No poverty, along with SDG 6: Safe water and sanitation and SDG 5: Gender equality on the CAWST team in Canada. Photo credit: ACGC.

 -Marcio providing online consulting support.
-Marcio providing online consulting support. -Lona facilitating online training.
-Lona facilitating online training.


 -A community health club gathers to visit households and learn about solutions for safe water, sanitation and hygiene near Ndola, Zambia
-A community health club gathers to visit households and learn about solutions for safe water, sanitation and hygiene near Ndola, Zambia
 -A community member of Abeshege, Ethiopia demonstrates her homemade handwashing station and proper technique. This photo was taken as part of a baseline study, against which we compared results from the subsequent phase of a Self-Help Group program. After one year, we saw significant improvements in practicing healthy behaviours and sharing knowledge with others.
-A community member of Abeshege, Ethiopia demonstrates her homemade handwashing station and proper technique. This photo was taken as part of a baseline study, against which we compared results from the subsequent phase of a Self-Help Group program. After one year, we saw significant improvements in practicing healthy behaviours and sharing knowledge with others.





 -Iván Castro, MSc, and Rocío Robayo, PhD, of FRPG deliver a presentation on safe water to Worley staff
-Iván Castro, MSc, and Rocío Robayo, PhD, of FRPG deliver a presentation on safe water to Worley staff -Worley team helps with biosand filter construction and installation in Cómbita
-Worley team helps with biosand filter construction and installation in Cómbita -Winners of the Worley Tippy Tap challenge, Fernando and Ashle
-Winners of the Worley Tippy Tap challenge, Fernando and Ashle
 Yashi facilitates an icebreaker activity to help students get more comfortable discussing WASH issues
Yashi facilitates an icebreaker activity to help students get more comfortable discussing WASH issues Yashi with school children after a workshop on addressing water scarcity
Yashi with school children after a workshop on addressing water scarcity




